

episode 1: a hard day's night (pt 1)
episode 1: a hard day's night (pt 1)
if surgery is a game, who's playing?

A note on structure: I'm going episode by episode as a way to begin slowly digging through the many layers of Grey's Anatomy. There's a lot here, though, so this essay is in two parts.
Here is what happens in the first episode of Grey’s Anatomy:
Dr. Meredith Grey (Ellen Pompeo) kicks a guy named Derek (Patrick Dempsey) out of her house. The night before, they’d met a bar and gone home together. Later, he turns out to be her boss: a guy named Dr. Derek Shepherd.
Meredith begins work as a surgical intern at Seattle Grace Hospital. She meets the other interns, as well as residents and attendings.
Meredith stumbles initially when working with her first patient, then successfully makes a difficult diagnosis.
Dr. George O’Malley (T.R. Knight) is picked to be the first intern to perform a surgery by himself. He starts confidently, then freezes.
Meredith visits her mother, Ellis (Kate Burton), who resides in an assisted living facility. We learn that Ellis - who used to be a surgeon, too - has now lost much of her memory.
And here are the first words of Grey’s Anatomy, spoken in voiceover by Meredith:
“The game. They say a person either has what it takes to play or they don’t. My mother was one of the greats. Me, on the other hand - I’m kind of screwed.”
We’ll get to why Meredith thinks she’s screwed later. For now, let’s focus on the fact that the very first lines of one of the most popular TV shows in the United States describe medicine — specifically surgery — as a game.
Let’s assume that this isn’t a one-off, that this mentality is common enough, and influential enough, among doctors to merit a closer look. Grey’s certainly thinks it is: “This is your starting line. This is your arena,” Chief of Surgery Dr. Richard Webber (James Pickens Jr.) says as he gives the new interns a tour of the operating rooms. “How well you play - that’s up to you.”
And let’s assume also that games are important. They can be fun and silly or all-consuming and violent, depending on the game itself, who’s playing, the rules and code of conduct, and the outcome of the match. War is sometimes called a game, too, and surgeons, like soldiers, wield weapons. In the words of Dr. Cristina Yang (Sandra Oh),
“Surgery is hot. It’s the Marines. It’s macho, it’s hostile, it’s hardcore.”
Referring to surgery as a game doesn’t mean it’s not being taken seriously. Athletes, like surgeons, ballet dancers, sculptors, musicians and chefs, are disciplined, hard-working and intensely invested in developing their skills to perfection. But an athlete playing a game has different priorities and faces different consequences from a doctor working with a patient.
What insights might we gain about surgery from it being described as a game?
The players are considered the most important participants because they’re the center of the action, and they drive the action. They decide where and how everything happens.
While the outcome of one big game might accelerate or slow the momentum of a player’s career, a player is usually measured by their own performance and contribution to the team, not by how the team does overall. However, a player who isn’t seen as contributing sufficiently to the team may be blamed for a loss, while players who are seen as contributing more might be subject to less sanction - on and off the field - due to their perceived importance.
Within teams, players often find themselves at odds due to competition for finite resources, which creates tension and distrust. However, meeting their goal requires them to collaborate well, because the game can only be won with considerable coordination, skill and practice - and because while they as individuals can perform better or worse, there is only one final score.
When players collaborate successfully, the victories are awe-inspiring. But when the results are losses, the competitive nature of the game makes it difficult for players to seek support from one another, particularly when they’re suffering from a lack of confidence. Perhaps for this reason, many otherwise excellent players struggle to work collaboratively.
A major problem with this metaphor, though, is that if the surgeons are the players - what does that make the patients? Are we simply the material with and on which the game is played? How are we supposed to change our final score if we’re not even on the field?
Most of the games we play require winners and losers, and the two groups are dependent on each other. Loss always benefits someone else. If someone doesn’t lose, someone else cannot win.
It’s not immediately clear why Meredith, our first and central player, thinks she’s screwed. She’s a talented doctor from a prestigious family and all the men are falling over themselves to talk to her.
But in a moment of vulnerability, she admits to George that though others see her mother in her, the Dr. Ellis Grey didn’t see herself in Meredith: “She tried to talk me out of [going to medical school]. Said I didn’t have what it takes to be a surgeon, that I’d never make it.”
There will be plenty to say later about Meredith and her mother, together and separately, as doctors and caregivers and ethical beings. For now, what I want to note is that the idea that someone might not ‘have what it takes’ to be a surgeon implies that there’s something specific but indefinable that makes a person able to perform surgery well. This specific but indefinable trait differentiates surgeons not just as individuals but as a distinct group separate from non-surgeons.
It may well be true that surgery requires a unique set of skills that are only accessible to some. But there are inherent risks in believing that only some people are capable of doing something. An indefinable standard might seem to exclude arbitrarily, but it will always be impossible for some people to meet; and that is where we so often find that the standard wasn’t arbitrary at all, but intentional, specific and discriminatory.
Becoming a doctor is a complicated and difficult process, and not just because of the work. Each step of training and round of examinations is highly regulated to ensure that every person who receives a license to practice medicine has met a certain set of standards. We’ll get more into how that system was developed later, because the history sheds some light on what exactly those standards were intended to be.
Essentially, though, our prospective doctors now would face a much less discriminatory and treacherous path if it weren’t also the case that acquiring a medical license is extremely expensive - and time-consuming, which increases the expense exponentially.
Further, a medical education can be a risky investment because there are so many occasions where a partially trained doctor can be rejected from further training. The rejection can be attributed to any number of reasons or factors, most of which boil down to just not being considered good enough.
A person wanting to go to medical school usually has to complete an undergraduate degree first, which takes 3-4 years. Medical school is another 4 years, at the end of which a student technically becomes a doctor but can’t yet practice. To gain clinical experience, they must be matched to a residency program, where they will begin as an intern - and pass more tests - before earning the title of ‘resident.’ Residencies range in length from 3-7 years; a surgical residency must be at least 5 years long.
In total, becoming a doctor takes at least a decade; and for most of that time, a person will be a full-time student, paying to work instead of being paid. As a result of this enormous cost, and risk, it is much easier for wealthy people to become doctors - which also means that it’s much easier for them to access power over certain resources, and power over other people’s bodies.
Not all medical graduates match into residency programs, though. In fact, thousands of qualified doctors go unmatched - some for years. I recommend reading this excellent Twitter thread by Dr. Bryan Levya, who explains how this employment deficit disproportionately impacts Black, Latinx and Indigenous doctors.

Modern healthcare did not arise organically, and exceptional minds do not rise naturally to the surface like bubbles. Instead, some people have maintained control over health resources and others have been prevented from receiving adequate healthcare. There’s no way to know if our current ‘class’ of surgeons represents the people best suited to hold a surgeon’s power, who most deserve to earn a surgeon’s salary - not incidentally, the highest average salary of any occupation in the United States.
A 2021 survey of surgical students, residents and faculty demonstrated that racial disparities begin with who applies to and enrolls in medical school, and they only grow more pronounced through residency and faculty appointments. The authors concluded that Black and Latinx Americans in particular were significantly underrepresented in the surgical workforce, which means that that workforce is “not optimally equipped to handle the needs of our increasingly diverse patient population.” They also noted that while there are many factors that maintain these disparities,
“One of the most vital and difficult parts of promoting diversity is in creating a culture of respect and inclusion. Surgery has long been structured as a hierarchical system. It is imperative that the individuals in positions of authority model positive behavior and promote inclusion.”1
Grey’s Anatomy has more nonwhite doctors than is statistically accurate in the U.S. - particularly more Black doctors, who make up 16 percent of the workforce on Grey’s.2
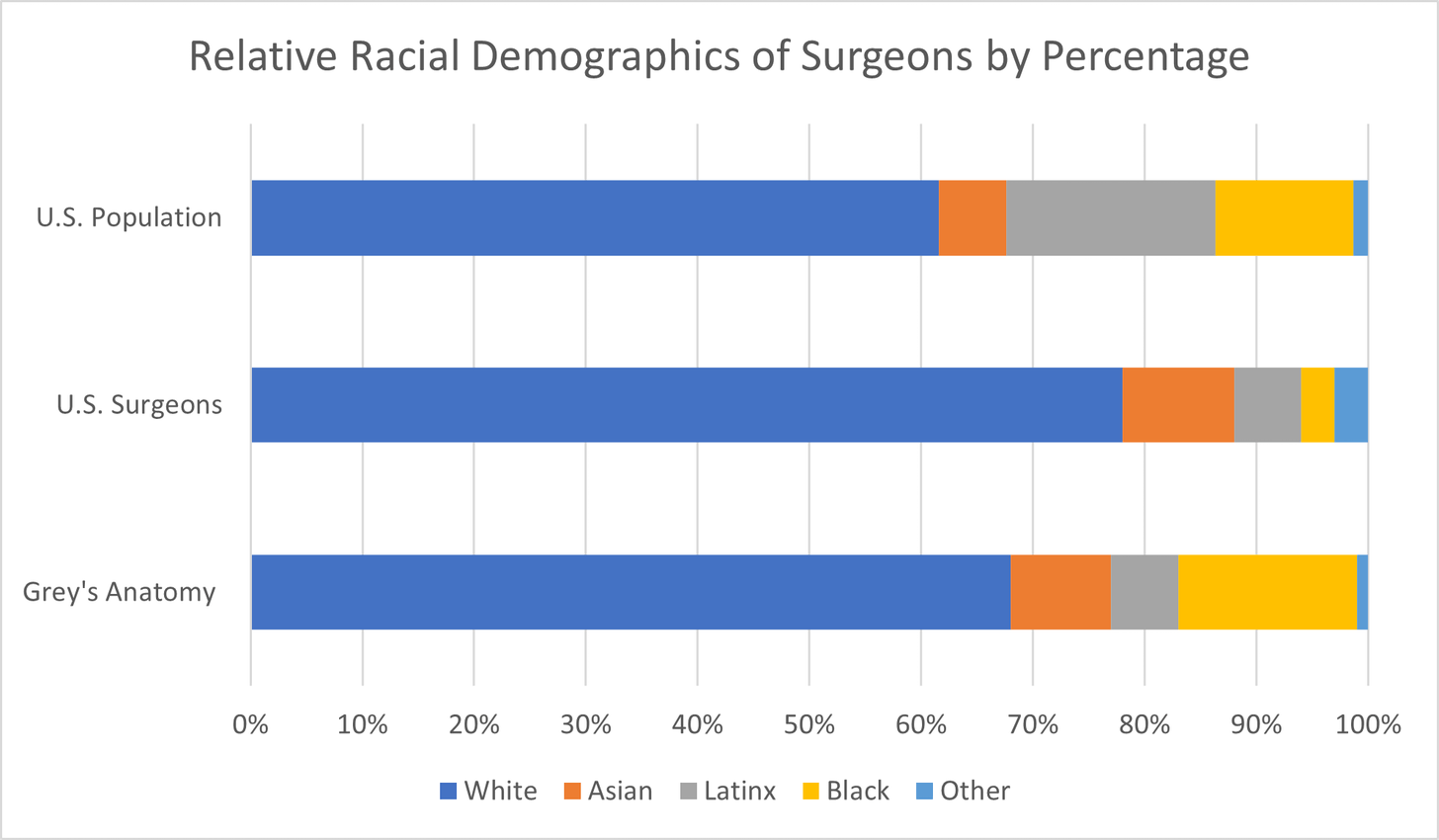
But the fact that Black Americans are underrepresented in the surgical workforce doesn’t necessarily mean that Black surgeons are overrepresented on Grey’s. It means that the show provides us with an opportunity to see American surgeons who accurately reflect our country.3
Dr. Miranda Bailey (Chandra Wilson), the resident in charge of our main group of interns, establishes in an introductory speech that hierarchy and suffering are both important parts of medical training. “You’re interns, grunts, nobodies, bottom of the surgical food chain,” she says. “You run labs, write orders, work every second night until you drop and don’t complain.”
Suffering and hierarchy may both be inevitable to some degree in medicine and education, as they seem to be in the rest of life. However, I think we can agree that there should be limits on, for example, how much suffering it is permissible to inflict for the sake of education in a professional environment.
When Dr. Preston Burke (Isaiah Washington), a cardiothoracic surgeon and attending, announces that he has selected George to be the first intern to perform a solo surgery - an honor, in Burke’s words, “reserved for the intern who shows the most promise” - George freezes, stunned. His disbelief suggests a lack of self-esteem, but I also suspect that George knows already that this chance is a test.
After all, Burke has just watched George repeatedly fail to place an IV line in a patient’s arm, stabbing him with the needle over and over. When Burke stepped in to place the IV, George - in an awkward attempt at camaraderie - said, “Bet you missed a lot when you first started out.” And Burke looked up, fixed him with a sardonic smile, then scoffed and said, “You and I are going to have so much fun together.”
In other words, George has no reason to think that Burke genuinely believes in his skill as a doctor - but why else would Burke let him cut someone open?
After Burke’s announcement, Bailey tries to convince him to change his mind, telling him that George isn’t his guy. “Every year you pick your guy,” she says, “and every year your guy suffers more than any other intern!”
But no, Burke is sure. He knows why he picked George: “Terrorize one and the rest fall in line,” he says.
The apparent desire to treat professional ‘inferiors’ disrespectfully is also reflected in the doctors’ habit of ignoring nurses - and when they’re not ignoring them, they often insult them. The doctors don’t experience consequence for this, either.
At the beginning of the first episode, Dr. Alex Karev (Justin Chambers) has incorrectly diagnosed the source of a patient’s fever. A nurse working with the patient presses him to think more deeply about his treatment plan. He says that he’s not interested in her opinion because she didn’t go to medical school. Then, when she’s barely out of earshot, he says, “God, I hate nurses.”
Though Alex will pay for his rudeness when his error is revealed in front of the Chief, the nurse won’t receive redress for the harassment - or acknowledgement for having been right. Meredith overhears the nurse’s comments to Alex, and she steps in to save the day.
It’s particularly aggravating because the nurses don’t return the doctors’ disdain: they offer help to the interns because they know they need help, even though those same doctors will not respect them after they get their bearings. Instead, the nurses will fade into the background, just a pair of hands and a surgical mask. They enable the surgeons’ work, so the surgeons understand them as necessary - but not as important.
On Grey’s and other medical dramas, we rarely see nurses doing the things they do in real life, and we certainly don’t see other important hospital staff such as porters and cleaners. In real life,
“Nurses manage patient conditions, prevent deadly errors, teach and advocate for patients, and work for better health systems. [And] patients die when nurses are understaffed or underempowered and when nursing care is assigned to those who are not nurses.”
This essential omission of key aspects of nursing contributes to the narrative coherence of nurses’ lower status on the show. Doctors, as a group, are allowed to openly demean nurses because their jobs are understood to be more important, which seems to justify them holding power. Nurses, on the other hand, must tolerate poor treatment because their jobs seem less important, which - for some - translates to them being less deserving of respect and shared resources.
But surgeons are dependent on nurses, because surgery cannot happen without nurses. It also can’t happen without cleaners, porters, anesthesiologists, technicians of all kinds, and all other healthcare staff who enable careful, thorough, effective patient care.
Grey’s Anatomy isn’t really about surgery, or what it takes to be a surgeon. It’s about desire, and desirability; wanting, whether for healing or intimacy or both. Wanting, desiring, yearning, and everything that people will do to fill the absence left by desire.
Consider the following quote from Grey’s executive producer Peter Horton, who also directed seven episodes, including this one:
“It was always about the relationships. It was primarily a story about Derek and Meredith, and longing…The opening scene of the piece is the two of them having just slept together in a one-night stand. Now, it was like, ‘We can’t be together because you’re my boss.’ That becomes the obstacle that the two of them have to negotiate with and dance around for, you know, years.”
I can appreciate a dance that goes on for years, particularly when the partners grow and mature as they learn to dance together. But a professional power imbalance isn’t just another obstacle on the way to happily-ever-after.
An imbalance of power, particularly in an intimate relationship, poses a risk to the person with less power, who may have less ability to meet their own needs for reasons of resources, experience or confidence. The more powerful person, meanwhile, may in fact benefit - even passively, subtly, or unconsciously - from their position of greater power, and might work - even passively, subtly, or unconsciously - to maintain that position.
Let’s look at the first conversation Meredith and Derek have at the hospital. When Meredith sees Derek and realizes who he is, she turns around and leaves the room she’s just entered. He follows her, grabs her arm, and pulls her into the stairwell.
That’s the first red flag. He doesn’t ask, doesn’t invite. He just grabs.
Meredith: Dr. Shepherd, we should pretend it never happened.
Derek: What never happened? You sleeping with me last night or you throwing me out this morning? Because both are fond memories I’d like to hold onto.
M: No, there will be no memories. I’m not the girl in the bar anymore and you’re not the guy. This can’t exist. You get that, right?
D: You took advantage of me and now you want to forget about it.
M: I did not!
D: I was drunk, vulnerable and good-looking, and you took advantage.
M: Okay, I was the one who was drunk, and you are not that good-looking.
D: Maybe not today. Last night? Last night I was very good-looking. I had my red shirt on, my good-looking shirt. You took advantage.
M: I did not take advantage.
D: Want to take advantage again - say, Friday night?
M: No. You’re an attending, and I’m your intern. Stop looking at me like that.
D: Like what?
M: Like you’ve seen me naked.
[Derek smiles.]
M: Dr. Shepherd, this is inappropriate. Has that ever occurred to you?
[Meredith leaves. Derek stands there looking confused.]
Two other important red flags:
Derek repeatedly ignores the boundaries that Meredith is setting. She sets them well: confidently and clearly. He ignores them.
When Derek jokes that Meredith took advantage of him, he is both minimizing and ridiculing the very idea of advantage. He is also preemptively dismissing the idea that there might be something inappropriate in his conduct by implying that they have equal power in this moment, and therefore equal culpability for whatever comes next.
Derek’s argument is that because they met on (presumably) equal footing - two good-looking, mildly intoxicated people in a bar - they can continue to be on equal footing in their personal relationship, even though they now also have a professional relationship. This implies both that it’s possible to firmly distinguish between personal and professional roles in a relationship, and that it’s possible to switch into ‘personal’ mode when firmly situated in a professional environment. This would mean that it’s not professionally inappropriate for him to pursue her romantically.
Now, Meredith’s beauty does give her power, as does her aloofness, talent and royal lineage, and I do think it’s important that they met and connected before Meredith started working at the hospital. Still, as she says, he’s an attending and she’s an intern - and he’s beautiful and talented too, not to mention magnetic. Meredith is powerful for an intern, but she does not have as much power as him, and his professional power specifically includes power over her and her career.
What that means is that there is never a time - not outside the hospital, and certainly not inside of it - when his professional role ceases to be relevant to their personal relationship.
In this conversation, Derek dismisses not just Meredith’s concerns, but her comfort and her consent, as well. He consistently prioritizes what he wants from her over what she wants out of the situation, and in doing so, prevents her from getting what she wants. This isn’t his goal, but it doesn’t seem to be a problem for him, either.
And yet - despite all this - Patrick Dempsey is so very charismatic and adorable that I hear his dialogue as funny and engaging, even when trying to parse the words. It’s hard not to dismiss behavior you don’t want to think about when you actually really like the character, not to mention the actor.
I’ve been listening to some Grey’s Anatomy podcasts, and this tension - discomfort plus the instinct to reduce or dismiss it - is clearly something a lot of us are struggling with.
From Pick Me Choose Me Podcast Me:
“I think Meredith handled this very well, I think she set clear boundaries, I think she was very professional…but Derek’s just so darn charming.”
“Totally inappropriate relationship, but still makes my heart melt, because MerDer.”
From The On-Call Room:
“I was really weirdly taken aback by that scene, because he’s so, like, undressing her with his eyes and being like very rape-y…Meredith calls it out, like, stop saying this, and he just keeps doing it. It’s like, I know his character, so I’m like aww, but if that - that’s like, very frightening.”
Last but not least, from Scalpels and Tequila:
“Back then I think it would’ve been looked at as, she’s playing hard to get, whereas today - hey, Derek, you’re sexually harassing a subordinate after she’s asked you to stop how many times?...He literally has her cornered on a stairwell and is in her personal space, and I remember thinking how, like, hot and heavy that was when I was younger, and now I’m looking at it like, You should’ve kneed him in the balls.”
I’m particularly struck by the phrase ‘I know his character.’ A character is a figure in a story - Dr. Derek Shepherd, performed by Patrick Dempsey. But character is also a person’s traits, qualities, reputation; and in fiction, the two meanings combine to indicate that the character of Derek is his listed qualities. And we can understand a character’s role in a story - what they do for the story, how their presence changes its direction - by examining how their qualities are presented.
Grey’s presents Derek as eminently trustworthy: he’s a doctor, he’s handsome, and he has a warm, steady gaze, all of which align with fairytale definitions of goodness. Rhimes has said that Derek was designed to be the ‘perfect man,’ and Dempsey plays that part well - he starred in seven rom-coms between 1987 and 2010, which is a long time for an actor (and their body) to continue to be seen as an ideal.
The problem with Derek’s ‘perfection’ - his princely charm and beautiful hair - is that they contribute heavily to how we interpret his actions. He often looks better than he is.
read pt 2 of this essay here.
Aggarwal et al. “Is There Color or Sex Behind the Mask and Sterile Blue? Examining Sex and Racial Demographics Within Academic Surgery.” Annals of Surgery, Vol. 273, no. 1, Jan. 2021.
David Lynn Painter, Alison Kubala and Sarah Parsloe. “Playing doctor on TV: physician portrayals and interactions on medical drama, comedy and reality shows.” Atlantic Journal of Communication, Vol. 28, no. 5, Nov.-Dec. 2020.